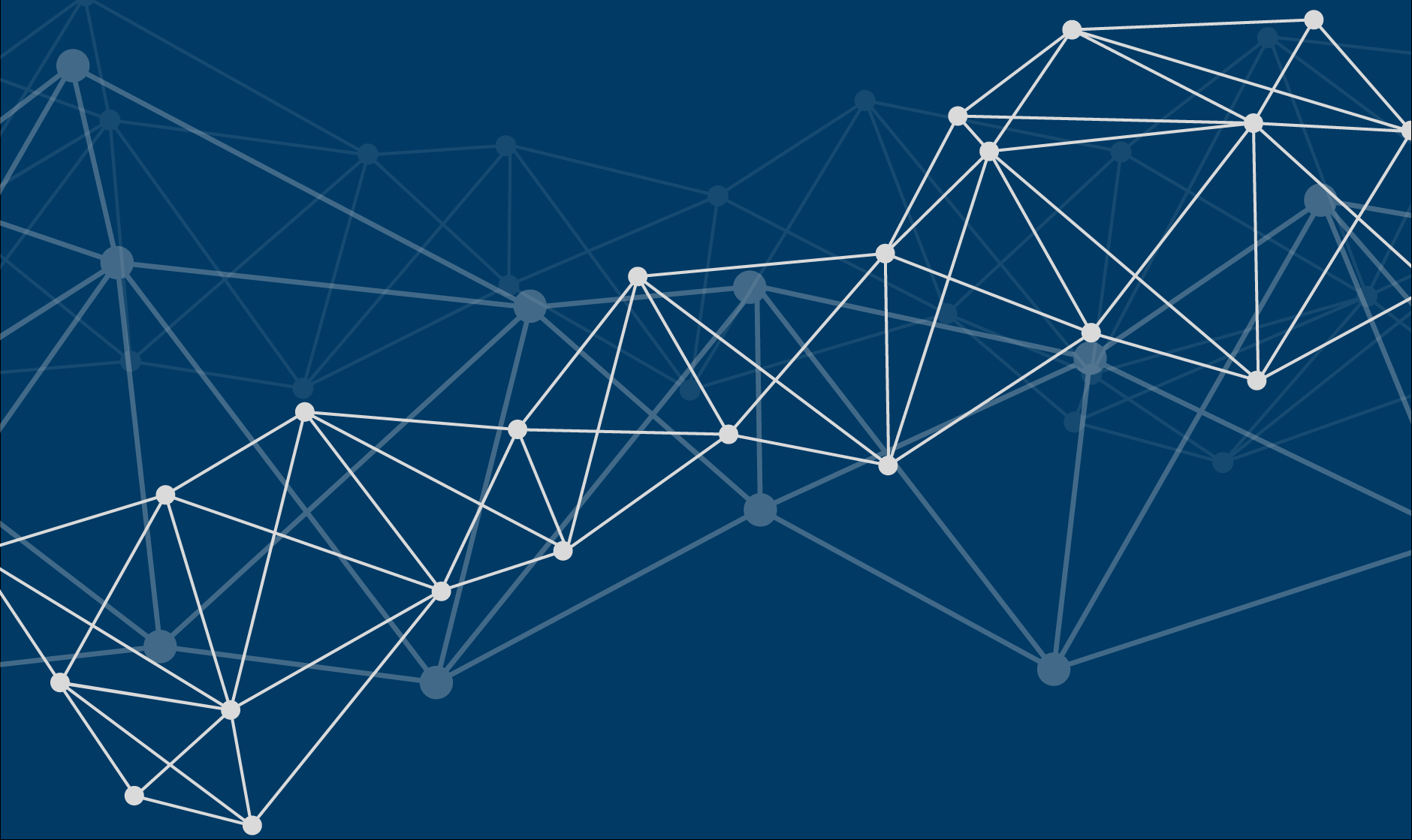

DEVELOPMENT PIPELINE
ALS (AMYOTROPHIC LATERAL SCLEROSIS)
Medical need in ALS
ALS is a motor neuron degenerative disease that affects both upper and lower motor neurons of the central nervous system. It is a progressive disease, with patients becoming increasingly dependent on family and carers ultimately leading to death. The average survival time is about three to five years. ALS has been divided into types: hereditary, which is known as familial ALS (fALS); and idiopathic, known as sporadic ALS (sALS). fALS affects around 5–10% of the ALS population and sALS the rest of the patients; however, while the origins are different, the symptoms and progression of the disease remain largely the same. These symptoms include physical impairment, increased saliva production, muscle weakness, loss of speech, poor posture, abnormal reflexes and respiratory problems.
The current number of patients in ALS is about 50.000 in the US and Europe in total with estimated new cases of 15.000 patients every year with an average survival time of 1 to 5 years after the first symptoms, depending on age and gen-mutation. Due to aging of the population a further increase of about 2% in average is assumed.
Globally the number of ALS cases is approximately 230.000 and is expected to increase to 380.000 in the next 20 years. The highest prevalence rates are in patients between 60 and 79 years of age.
There are only two therapeutic options in the market at this moment. Riluzole, the standard of care in many countries and shown to delay disease progression by 5% and RADICAVA, only available in the USA and shown to reduce disease progression by 15% in some ALS subtypes, at a cost of more than US$100.000 a year.
Pathophysiological mechanisms implicated in ALS
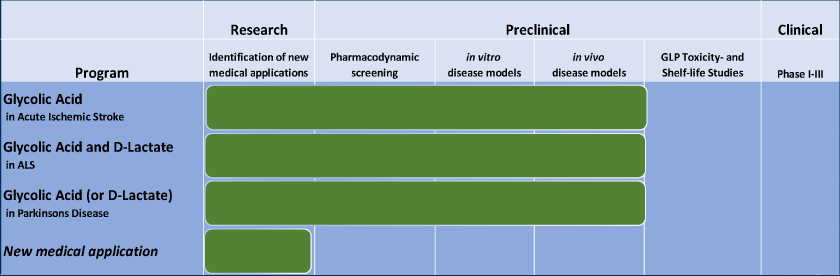
ALS is linked to increased intracellular calcium, impaired mitochondrial transport, and mitochondrial dysfunction.
ALS leads to:
- Mitochondrial damage and dysfunction
- Increased intracellular calcium
- ER Stress
that play an important role in the evolution of these diseases and ultimately induce neuronal cell death.
NEUREVO Results in ALS

- Motor neurons from ALS patients
- Four ALS patients (first-in-man human study)
✔ very good rescue of neuronal phenotype
✔ 3 out of 4 of patients responded
✔ delay of disease progression
✔ no toxicity*
STROKE
Medical need in stroke
Annually, 15 million people worldwide suffer from a stroke. Thereof 5 million die and another 5 million are left permanently disabled, placing a burden on family and community. Stroke is uncommon in people under 40 years. The major risk factors for stroke are similar to those for coronary heart disease; with high blood pressure and tobacco use the most significant modifiable risks. The incidence of stroke is declining in many developed countries, largely as a result of better control of high blood pressure, and reduced levels of smoking. However, the absolute number of strokes continues to increase because of the ageing population.
Only in the USA and Europe approximately 1,9 million inhabitants suffered a stroke each year with an expected annual increase of about 1,4%.
Stroke is caused either by a blockage in the blood flow in a cerebral artery and thus in the oxygen and food supply to the brain supplied by this vessel or by a reduction in the global blood supply to the brain (e.g. during a heart infarct or during an abrupt disminution of the blood pressure), the so-called anoxia/hypoxia brain damage. The undersupply causes brain cells to die, which leads to lasting motor damage. Whereas in hypoxic brain damage the whole brain is affected, in single vessel ischemic stroke two ischemic regions are distinguished: the region that is supplied by the affected vessel alone (core) and the surrounding region that is indirectly supplied by other vessels (penumbra). In the core region, brain cells are damaged after only a few minutes due to the complete interruption of the supply. The brain cells in the penumbra are only affected after a longer time due to an undersupply.
There are currently 2 treatment possibilities for a stroke:
- Fibrinolysis: the blood clot is dissolved using «recombinant tissue plasminogen activator» (rtPA). This causes the vessel to reopen.
- Mechanical reopening of the artery: the blood clot is removed mechanically, i.e. by an intraoperative manual procedure.
These treatments prevent to a certain extend the spread of the ischemic damage to the penumbra, but can also cause further damage, the so-called ischemic-reperfusion damage. None of these treatments has a neuroprotective effect, i.e. these procedures cannot prevent the death of the pre-damaged neurons, e.g. in the ischemic nucleus.
The currently available drugs do not effectively improve clinical outcome in stroke patients. There is an immense opportunity to come up with effective neuroprotective or neurorestorative treatments in the space of acute ischemic stroke and anoxic/hypoxic brain damage.
Pathophysiological mechanisms implicated in stroke
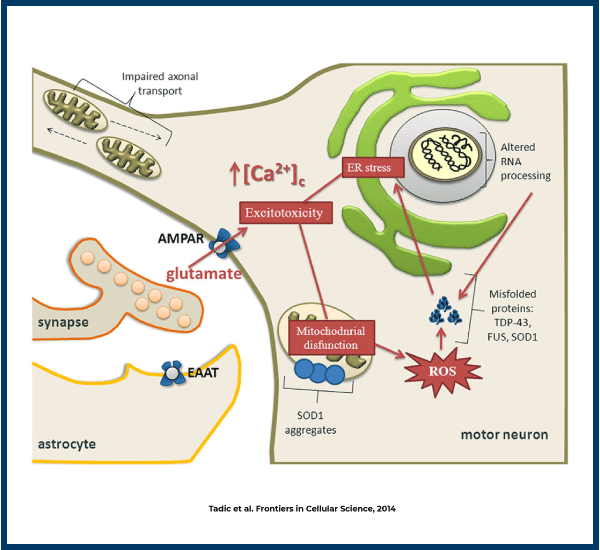
Stroke induces increases in intracellular calcium, decreases ATP production and activates apoptosis.
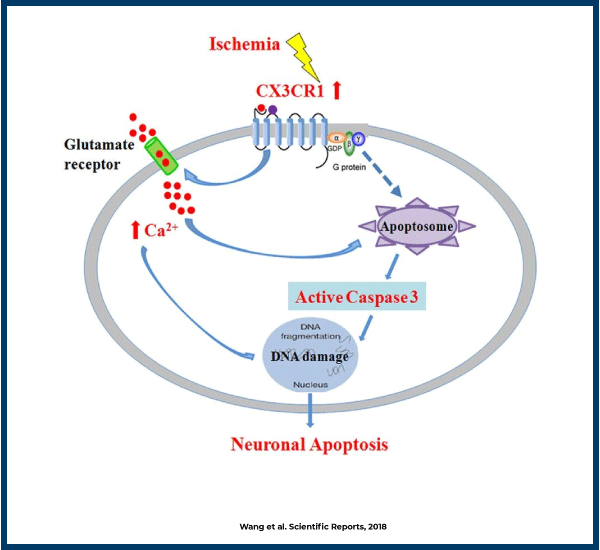
Stroke leads to:
- Mitochondrial damage and dysfunction
- Increased intracellular calcium
that play an important role in the evolution of these diseases and ultimately induce neuronal cell death.
NEUREVO Results in Stroke
Three animal models:
- Global ischemia (Prof. Plesnila, Intitute for Stroke and Dementia)
- Middle cerebral artery occlusion (Prof. Meisel, Charité)
- Endovascular swine model (Prof. Janowski and Prof. Walczak, University of Maryland)
✔ up to full protection
✔ very good motor function recovery
✔ no toxicity*
PARKINSON´S DISEASE (PD)
Medical need in PD
PD is the second most common chronic progressive neurodegenerative disorder in the elderly after Alzheimer’s disease, affecting 1–2% of individuals ages over 65 years.
The USA and Europe accounted for about 2 million cases in total with estimated new cases every year of about 125.000. Worldwide more than 10 million people are living with PD. Due to ageing an annual increase is expected for about 3% on average over USA and Europe.
PD leads to movement problems. While the exact cause of PD is unknown, it may include a number of factors such as aging, environmental factors/exposures, and genetic predispositions. Studies carried out in this field have concluded that environmental stress and genetic predispositions accelerate the aging process in the CNS, and that the motor symptoms of PD start when dopamine loss passes a threshold amount. Current treatments are symptomatic and focus on the management of dopamine levels in the brain, with levodopa-based therapies remaining the standard of care. However, the effectiveness of levodopa declines with time and complications such as wearing off (ON-OFF syndrome), levodopa-induced dyskinesia, and Parkinson’s psychosis arise. Treatment for these complications remains one of the major unmet needs in PD with limited effective treatment options.
Pathophysiological mechanisms implicated in PD
Parkinson’s disease is also linked to increased intracellular calcium levels and mitochondrial impairment.
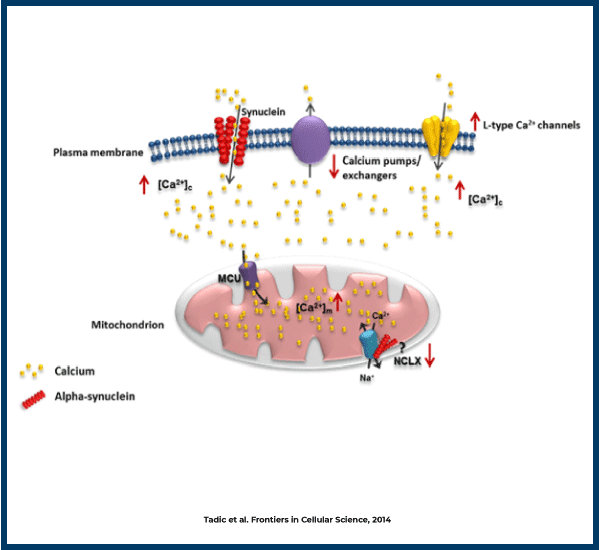
Parkinson´s disease:
- Mitochondrial damage and dysfunction
- Increased intracellular calcium
that play an important role in the evolution of these diseases and ultimately induce neuronal cell death.
NEUREVO Results in Parkinson
- One toxin-induced animal model
✔ very good neuroprotective effect
✔ no toxicity*
SPERM MOTILITY
Medical need in sperm motility
Worldwide, around 60 to 80 million couples are affected by infertility, and the rates vary from country to country. Increases in the global prevalence of infertility is a significant clinical problem. Around 8% to 12% of couples have to deal with the problem of infertility worldwide. Of all cases, about 40% to 50% of cases is due to male factor infertility. This may be due to one or combination of factors, such as abnormal morphology, lower sperm concentration, and poor sperm motility.
Sperm motility is the ability of sperm to move efficiently. This is important in fertility because sperm need to move through the woman’s reproductive tract to reach and fertilize the egg cell. Poor sperm motility can be a cause of male factor infertility.
Increasing infertility rate across the globe have led to the adoption of assisted reproductive technologies (ARTs). ARTs cover a wide spectrum of infertility treatments and offer solutions for males facing problems, such as low sperm count, abnormal sperm quality, and poor motility. ARTs consist mainly in three methods:
- Insemination: this method places sperm directly in the uterus. Like this sperm cells do not have to go thought the cervix, the main obstacle in their way to the egg cell. This method requires fairly good sperm motility, as sperm cells need to find the egg cell and fertilize it.
- In vitro fertilization (IVF): this method is more expensive than the previous one (ca. 12.000 Euros per cycle) and is performed in a dish. Sperm cells and the egg cell are place in a dish for fertilization to take place. After that the fertilized egg is implanted back in the uterus to attach. This method also requires a certain degree of sperm motility, as sperm cell still need hyperactivate in order to fertilize the egg.
- Intracystoplamic Sperm Injection (ICSI): this method is the most expensive one and it needs to be performed by a specialized technician. Sperm cells are manually selected and injected directly in the egg cell. Sperm cells are not required to be motile.
However, these methods require hormonal treatments to obtain the oocyte, are very invasive, expensive and do not treat the real problem, namely the alterations leading to poor sperm motility.
Pathophysiological mechanisms implicated in alterations in sperm motility
Increasing male infertility has been linked to the exposure to environmental toxins, stress and an unhealthy life-style.
Factor affecting sperm motility (Dcunha, R. et al. Current Insights and Latest Updates in Sperm Motility and Associated Applications in Assisted Reproduction. Reprod. Sci. (2020))
These factors reduce the quality of the sperm by:
1) altering mitochondrial function/energy production of sperm cells and
2) increasing oxidative stress.
NEUREVO Results in sperm motility

✔ Increases sperm motility in human, bull and pig sperm
✔ This increase in sperm motility is maintained in time for at least 90 min.
* Data obtained from mice in laboratory and in monitored individual experimental treatments using a specific formulation. The ingestion of both substances can be toxic if used improperly and without the appropriate formulation. GLP-toxicity studies and Phase I/IIa toxicity and effectivity studies in humans are still pending. We advise against uncontrolled self-administration through the patients.